Preparing for this Test
The Adrenal Stress Profile test preparation contains information on cortisol and DHEA collection considerations, impact of glucocorticoids, and altered sleep-wake schedules.
Medications and Supplements May Impact Results
Should a patient discontinue a medication or supplement prior to testing?
Genova never recommends that patients discontinue medically necessary medications or supplements in order to complete testing.
There may be times when a patient may stay on a medication or dietary supplement during testing in order to evaluate its effectiveness, especially if a long-term medication. Discontinuing a substance is intended to establish a baseline finding. If you choose to discontinue a medication, a good rule of thumb is to take the biological half-life of the drug times 5 to allow for 'clearance' before testing. With certain medications, the drug itself may have cleared the body, but the effect of the medication may be longer lasting.
How will a medication or supplement impact hormone levels?
In many instances, it is unknown what potential impact a medication or supplement may have on test results.
Any questions regarding a medication or supplement impact on biomarker results can be researched by contacting the manufacturer, pharmacist, and/or searching the literature (PubMed, Google Scholar) for relevant information. Drug databases such as drugs.com, rxlist.com, Epocrates, and pdr.net, or laboratory textbooks such as Fischbach's A Manual of Laboratory and Diagnostic Tests may provide additional information.
Medication Interferents
The medications listed below are direct interferants to hormone assays resulting in falsely low or falsely elevated findings. Testing may not be appropriate for patients who cannot discontinue these medications.
| Interfering Medications/ Supplements |
Possible Impact on Results |
| Immunotherapy (i.e., cancer, autoimmune, and other condition treatments) |
Immunotherapy or diagnostic procedures utilising immunoglobulins or immunoglobulin fragments may produce antibodies that interfere with immunoassays. Such interfering antibodies may cause erroneous results.1
For additional information, visit the section on 'Immunoassay Interferents' below.
|
| Steroids |
Different steroids have differing effects on hormone levels, with some being direct assay interferents.2,3 See Adrenal Stress Profile test preparation for more info.
|
Immunoassay Interferents
For all assays utilising antibodies (i.e., immunoassays), the possibility exists for interference by heterophile antibodies in the patient sample. Patients who have regularly been exposed to animals or have received immunotherapy or diagnostic procedures utilising immunoglobulins or immunoglobulin fragments may produce antibodies, e.g. HAMA, that interfere with immunoassays. Such interfering antibodies may cause erroneous results. Additionally, rheumatoid factor, endogenous alkaline phosphatase, fibrin and proteins capable of binding to alkaline phosphatase can act as interferants.1 The following article thoroughly discusses hormone immunoassay interference: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8368230/
- Profiles using immunoassays include:
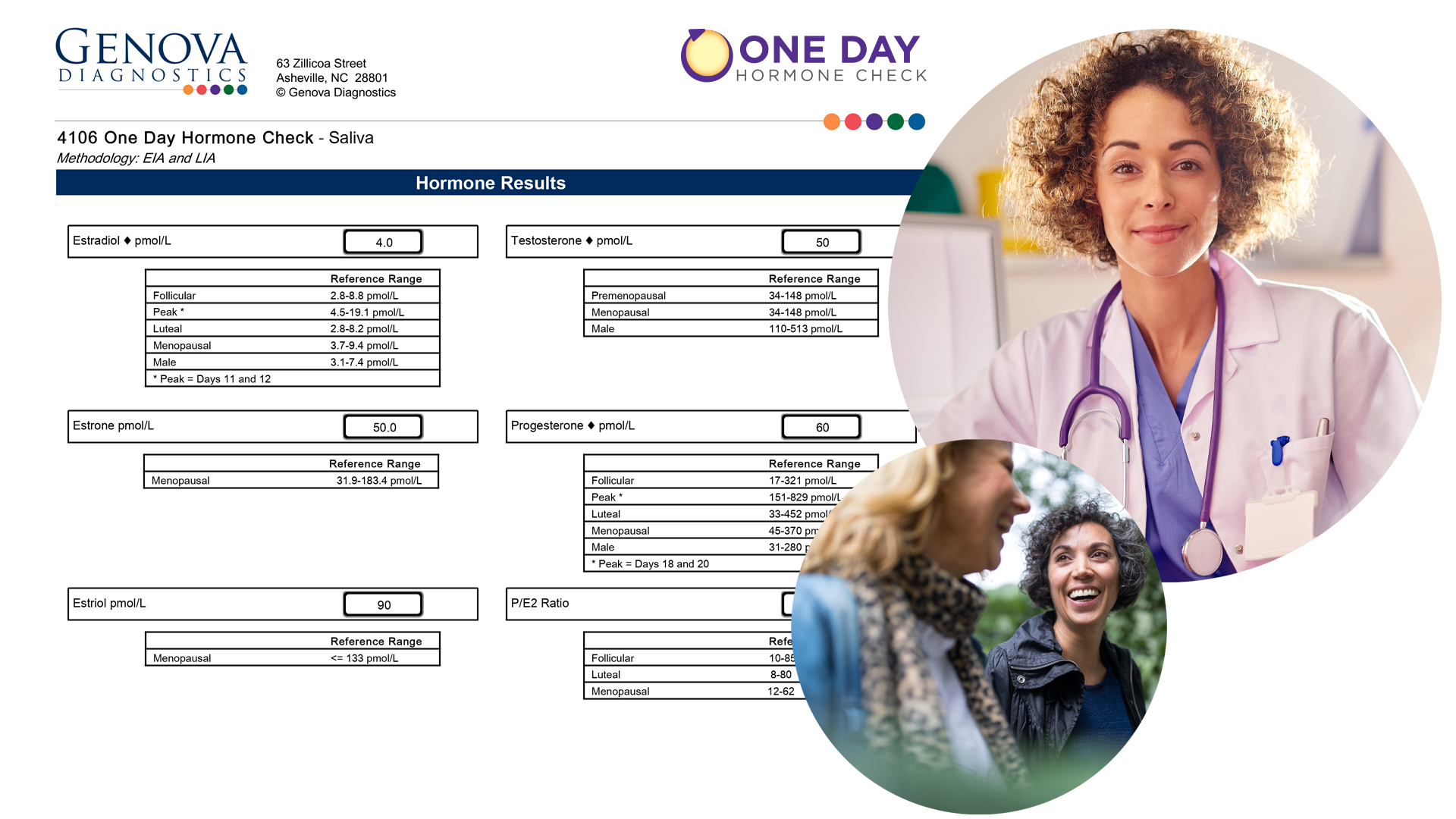
- Salivary hormones E1, E2, E3, P, T, cortisol, DHEA, melatonin
- Serum hormones E1, E2, E3, P, T, DHEAs, SHBG
- Thyroid Panel
Medication Influencers
The medications listed below will not interfere with Genova's ability to run the assays but may influence biomarker levels.
| Influencing Medications/ Supplements |
Possible Impact on Results |
| Ketoconazole, antibiotics, cimetidine, fibrates (gemfibrozil), metformin, statins, antiepileptics, digoxin |
These are examples of medications that are generally prescribed for non-hormone related conditions that can alter hormone levels and/or metabolism.2-19 This list is not exhaustive.
There is no recommendation to discontinue.
|
| Leuprolide, clomiphene, aromatase inhibitors (Anastrozole, Letroxole, Exemestane), tamoxifen, finasteride, spironolactone |
These are examples of medications that are generally prescribed to intentionally alter hormone levels and/or metabolism.2,3,17,20-28 This list is not exhaustive.
There is no recommendation to discontinue.
|
| Hormone Replacement Therapy (HRT) |
Genova's assays detect bio-identical hormones, but not synthetic or non-bioidentical hormones. Synthetic hormones, such as those from oral contraceptives, are generally not recommended for any of Genova's sex steroid hormone testing platforms - blood, urine, or saliva. Synthetic hormones may create unpredictable results that often do not reflect the patient's physiologic levels.
For additional information, visit the section on 'Hormone Therapy and Test Considerations' below.
|
Hormone Therapy and Testing Consideration FAQs
When should my patient take their hormones prior to testing?
The answer depends on several factors including the hormone delivery type, dosing intervals, specimen type, what information the clinician is hoping to glean, etc. In general, many clinicians opt to test their patients 8-12 hours following their last dose of hormones. Some clinicians wait 24 hours following transdermal cream application.
Published standardised guidelines and best practices are lacking regarding timing of supplementation with testing. The time to reach peak and trough levels, as well as time to steady state varies with each hormone and hormone delivery method. Furthermore, peak and trough levels may vary depending on the sample type evaluated (saliva, blood, urine). Pharmacokinetic studies exist for FDA-approved hormone products and provide information about half-life and time to steady state. The same kinds of studies do not exist for custom compounded hormones, making it challenging to know the best time to test. Most of the published literature utilises serum to conduct the pharmacokinetic studies; information on half-life and timing of saliva or urine sampling is sparse. Some sources suggest that measuring the trough level is ideal.
Can custom compounded bioidentical hormones be monitored with testing?
Many clinicians prefer to monitor patients on custom compounded formulas so they can adjust accordingly. Hormone compounding can result in variations depending on the base ingredients as well as actual dose of the active hormone. Genova has observed erroneously elevated levels of hormones in patients particularly being prescribed custom compounded formulations. These erroneous levels are not typically observed in baseline, unsupplemented samples. It is important to work closely with your compounding pharmacist to understand the formulations, pharmacokinetics, and pharmacodynamics. Pharmacokinetic studies exist for FDA-approved bioidentical hormones and provide information about half-life and time to steady state. These studies are sparse for custom compounded hormones. Blending more than one hormone in a regimen is another variable that affects the drug's kinetics, potentially resulting in unpredictable findings.
What impact does hormone cream have on testing?
Hormone creams tend to be underrepresented in serum and overrepresented in salivary samples. Progesterone is very lipophilic and accumulates in subcutaneous fat cells. Red blood cells passing through the capillaries play a role in transporting progesterone to salivary glands and other tissues.29 As such, we can see elevated progesterone in salivary samples for several months after complete cessation of transdermal therapy, before the progesterone depot is depleted. The degree of impact that transdermal hormone therapies may have on an individual's salivary hormone levels are determined by many factors: dose, route of administration, site of administration, pharmacokinetics of the preparation, patient compliance, adiposity, and patient metabolic individuality. Anecdotally, we have noticed salivary progesterone levels persisting for up to a year after discontinuation of transdermal creams in some patients.
Additionally, creams can directly contaminate samples. For example, a vaginal hormone cream can contaminate a urine sample. Residual cream on the fingers after application can contaminate tube caps, lips, or mouth before spitting into a tube. Sublingual hormones can directly contaminate salivary collections if they haven't been fully absorbed.
Can a patient test while taking synthetic, non-bioidentical hormones?
Synthetic hormones, such as those from oral contraceptives, are generally not recommended for any of Genova's sex steroid hormone testing platforms - blood, urine, or saliva. The assays are not designed to detect the molecular structure of synthetic hormones, only bio-identical and endogenously produced hormones. Synthetic hormones may create unpredictable results that often do not reflect the patient's physiologic levels. Hormone therapy impacts the hypothalamic-pituitary-gonadal axis via negative feedback as well as affecting binding protein levels, which then results in altered levels of endogenous hormones.30 Testing while on synthetic, non-bioidentical hormones may produce results that are not clinically useful.
How long after discontinuing oral contraceptives can a patient test hormone levels?
Prior to testing, it is preferred that there be at least two menstrual bleeds after discontinuing contraception (i.e., oral contraceptive pill, depo-medroxy-progesterone acetate, hormonal IUD like Mirena or Kyleena, etc.).31-33 Testing sooner may not assess the natural baseline menstrual cycle as the body needs time to readjust. Recent discontinuation of oral contraceptives may delay ovulation and prolong the follicular phase and thus overall cycle length.31 The overall duration of contraceptive use does not significantly affect the return of fertility after discontinuation.34
Unintentional hormone exposure can elevate levels
Patients should be instructed to avoid skin-to-skin exposure with close friends/family members that use hormone creams to avoid unintentional exposure. Exposure can be from close contact with others using prescription or over the counter transdermals including family members or occupational (i.e., massage therapy, pharmacies, health care facilities), and exposure to items that a person using transdermals touched including gym equipment, towels, doorknobs, sheets, etc.35,36 Anti-aging, anti-wrinkle creams, and other cosmetics and body care products may contain hormones even if not disclosed on the label. Additionally, over-the-counter products containing hormones can be purchased directly by consumers.37,38
Bleeding Gums and Salivary Testing
Salivary samples visibly contaminated with blood should be recollected. This can result in a false elevation of hormones. Blood concentrations of steroid hormones are several-fold higher than saliva levels.39,40 For this reason, brushing and flossing is discouraged for 1 hour prior to salivary collection. Additionally, if the patient has a condition that causes gums to bleed easily, such as gingivitis or periodontitis, or has dentures and other oral appliances, a plan should be in place to ensure gums do not bleed during testing.
Paediatric Patients
The reference ranges for all of Genova's endocrine profiles are based off a healthy cohort of patients aged greater than 18. Genova does not have pediatric reference ranges. A literature search may provide further insight into pediatric reference ranges.
REFERENCES
- Instructions for Use Beckman Coulter Access Immunoassay Systems;2020.
- Fishbach F. A Manual of Laboratory and Diagnostic Tests. 11th ed: Wolters Kluwer; 2022.
- Sarne D. Effects of the Environment, Chemicals and Drugs on Thyroid Function. In: Feingold KR, Anawalt B, Boyce A, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc; 2000.
- Castinetti F, Guignat L, Giraud P, et al. Ketoconazole in Cushing's disease: is it worth a try? J Clin Endocrinol Metab. 2014;99(5):1623-1630.
- Pont A, Williams PL, Azhar S, et al. Ketoconazole blocks testosterone synthesis. Arch Int Med. 1982;142(12):2137-2140.
- Medda F, Puligheddu P, Parodo G, et al. Short term treatment with ketoconazole: effects on gonadal and adrenal steroidogenesis in women. Clin Exp Obst Gynecol. 1987;14(3-4):161-166.
- Trachtenberg J, Zadra J. Steroid synthesis inhibition by ketoconazole: sites of action. Clin Invest Med. 1988;11(1):1-5.
- Adlercreutz H, Pulkkinen MO, Hämäläinen EK, Korpela JT. Studies on the role of intestinal bacteria in metabolism of synthetic and natural steroid hormones. J Steroid Biochem. 1984;20(1):217-229.
- Kwa M, Plottel CS, Blaser MJ, Adams S. The Intestinal Microbiome and Estrogen Receptor-Positive Female Breast Cancer. J Nat Cancer Inst. 2016;108(8).
- Galbraith RA, Michnovicz JJ. The effects of cimetidine on the oxidative metabolism of estradiol. NEJM. 1989;321(5):269-274.
- Bohnet HG, Greiwe M, Hanker JP, Aragona C, Schneider HP. Effects of cimetidine on prolactin, LH, and sex steroid secretion in male and female volunteers. Acta endocrinol. 1978;88(3):428-434.
- Barbara L, Corinaldesi R, Pasquali R, Raiti C, Zurita J, Stanghellini V. Endocrine effects of the H2-receptor antagonists cimetidine and ranitidine. Int J Tissue React. 1983;5(4):387-392.
- Hautanen A, Mänttäri M, Manninen V, Adlercreutz H. Gemfibrozil treatment is associated with elevated adrenal androgen, androstanediol glucuronide and cortisol levels in dyslipidemic men. J Steroid Biochem Mol Biol. 1994;51(5-6):307-313.
- Cai T, Hu Y, Ding B, et al. Effect of Metformin on Testosterone Levels in Male Patients With Type 2 Diabetes Mellitus Treated With Insulin. Front Endocrinol. 2021;12:813067.
- Campagnoli C, Berrino F, Venturelli E, et al. Metformin decreases circulating androgen and estrogen levels in nondiabetic women with breast cancer. Clin Breast Cancer. 2013;13(6):433-438.
- Meenakumari KJ, Agarwal S, Krishna A, Pandey LK. Effects of metformin treatment on luteal phase progesterone concentration in polycystic ovary syndrome. Brazil J Med Biol Res. 2004;37(11):1637-1644.
- Almalki HH, Alshibani TM, Alhifany AA, Almohammed OA. Comparative efficacy of statins, metformin, spironolactone and combined oral contraceptives in reducing testosterone levels in women with polycystic ovary syndrome: a network meta-analysis of randomized clinical trials. BMC Women Health. 2020;20(1):68.
- Stoffer SS, Hynes KM, Jiang NS, Ryan RJ. Digoxin and abnormal serum hormone levels. JAMA. 1973;225(13):1643-1644.
- Kley HK, Müller A, Peerenboom H, Krüskemper HL. Digoxin does not alter plasma steroid levels in health men. Clin Pharmacol Therap. 1982;32(1):12-17.
- Schmidt PJ, Martinez PE, Nieman LK, et al. Premenstrual Dysphoric Disorder Symptoms Following Ovarian Suppression: Triggered by Change in Ovarian Steroid Levels But Not Continuous Stable Levels. Am J Psych. 2017;174(10):980-989.
- Wheeler KM, Sharma D, Kavoussi PK, Smith RP, Costabile R. Clomiphene Citrate for the Treatment of Hypogonadism. Sex Med Rev. 2019;7(2):272-276.
- Glazener CM, Coulson C, Lambert PA, et al. Clomiphene treatment for women with unexplained infertility: placebo-controlled study of hormonal responses and conception rates. Gynecol Endocrinol. 1990;4(2):75-83.
- Geisler J, Detre S, Berntsen H, et al. Influence of neoadjuvant anastrozole (Arimidex) on intratumoral estrogen levels and proliferation markers in patients with locally advanced breast cancer. Clin Cancer Res. 2001;7(5):1230-1236.
- de Ronde W, de Jong FH. Aromatase inhibitors in men: effects and therapeutic options. Reprodud Biol Endocrinol. 2011;9:93.
- Lum SS, Woltering EA, Fletcher WS, Pommier RF. Changes in serum estrogen levels in women during tamoxifen therapy. Am J Surg. 1997;173(5):399-402.
- Jordan VC, Fritz NF, Langan-Fahey S, Thompson M, Tormey DC. Alteration of endocrine parameters in premenopausal women with breast cancer during long-term adjuvant therapy with tamoxifen as the single agent. J Nat Cancer Inst. 1991;83(20):1488-1491.
- Birzniece V, Sata A, Sutanto S, Ho KK. Neuroendocrine regulation of growth hormone and androgen axes by selective estrogen receptor modulators in healthy men. J Clin Endocrinol Metab. 2010;95(12):5443-5448.
- Rozner RN, Freites-Martinez A, Shapiro J, Geer EB, Goldfarb S, Lacouture ME. Safety of 5α-reductase inhibitors and spironolactone in breast cancer patients receiving endocrine therapies. Breast Cancer Res Treat. 2019;174(1):15-26.
- Stanczyk FZ, Paulson RJ, Roy S. Percutaneous administration of progesterone: blood levels and endometrial protection. Menopause. 2005;12(2):232-237.
- Simon JA. Estrogen replacement therapy: effects on the endogenous androgen milieu. Fertility Sterility. 2002;77 Suppl 4:S77-82.
- Najmabadi S, Schliep KC, Simonsen SE, Porucznik CA, Egger MJ, Stanford JB. Menstrual bleeding, cycle length, and follicular and luteal phase lengths in women without known subfertility: A pooled analysis of three cohorts. Paed Perinat Epidemiol. 2020;34(3):318-327.
- Balogh A, Ditrói F, Lampé LG. LH, FSH, estradiol and progesterone levels after discontinuation of hormonal contraception. Acta Univ Palack Olomucen Facult Med. 1981;101:95-101.
- Davis AR, Kroll R, Soltes B, Zhang N, Grubb GS, Constantine GD. Occurrence of menses or pregnancy after cessation of a continuous oral contraceptive. Fertility Sterility. 2008;89(5):1059-1063.
- Girum T, Wasie A. Return of fertility after discontinuation of contraception: a systematic review and meta-analysis. Contracep Reprod Med. 2018;3:9.
- Franklin SL. Effects of unintentional exposure of children to compounded transdermal sex hormone therapy. Ped Endocrinol Rev. 2011;8(3):208-212.
- Busse KL, Maibach HI. Transdermal estradiol and testosterone transfer in man: existence, models, and strategies for prevention. Skin Pharmacol Physiol. 2011;24(2):57-66.
- Gottswinter JM, Korth-Schütz S, Ziegler R. Gynecomastia caused by estrogen containing hair lotion. J Endocrinol Invest. 1984;7(4):383-386.
- Hermann AC, Nafziger AN, Victory J, Kulawy R, Rocci ML, Jr., Bertino JS, Jr. Over-the-counter progesterone cream produces significant drug exposure compared to a food and drug administration-approved oral progesterone product. J Clin Pharmacol. 2005;45(6):614-619.
- Hofman LF. Human saliva as a diagnostic specimen. J Nutr. 2001;131(5):1621s-1625s.
- Granger DA, Taylor MK. Saliv Biosci. Springer Nature; 2020.